Sterile pustules that settle on an erythematous-edematous base
DOI:
https://doi.org/10.47196/da.v30i1.2527Abstract
A 73-year-old patient, with a history of type 2 diabetes mellitus, high blood pressure, hypothyroidism, heart failure, dyslipidemia and obesity, medicated with enalapril, metformin and levothyroxine, attended the Dermatology Service for generalized pruritic dermatosis, which had been going on for 48 hours. after starting treatment with amoxicillin/clavulanic acid, on external guard, due to a presumed infected ulcer in the distal third of the right leg.
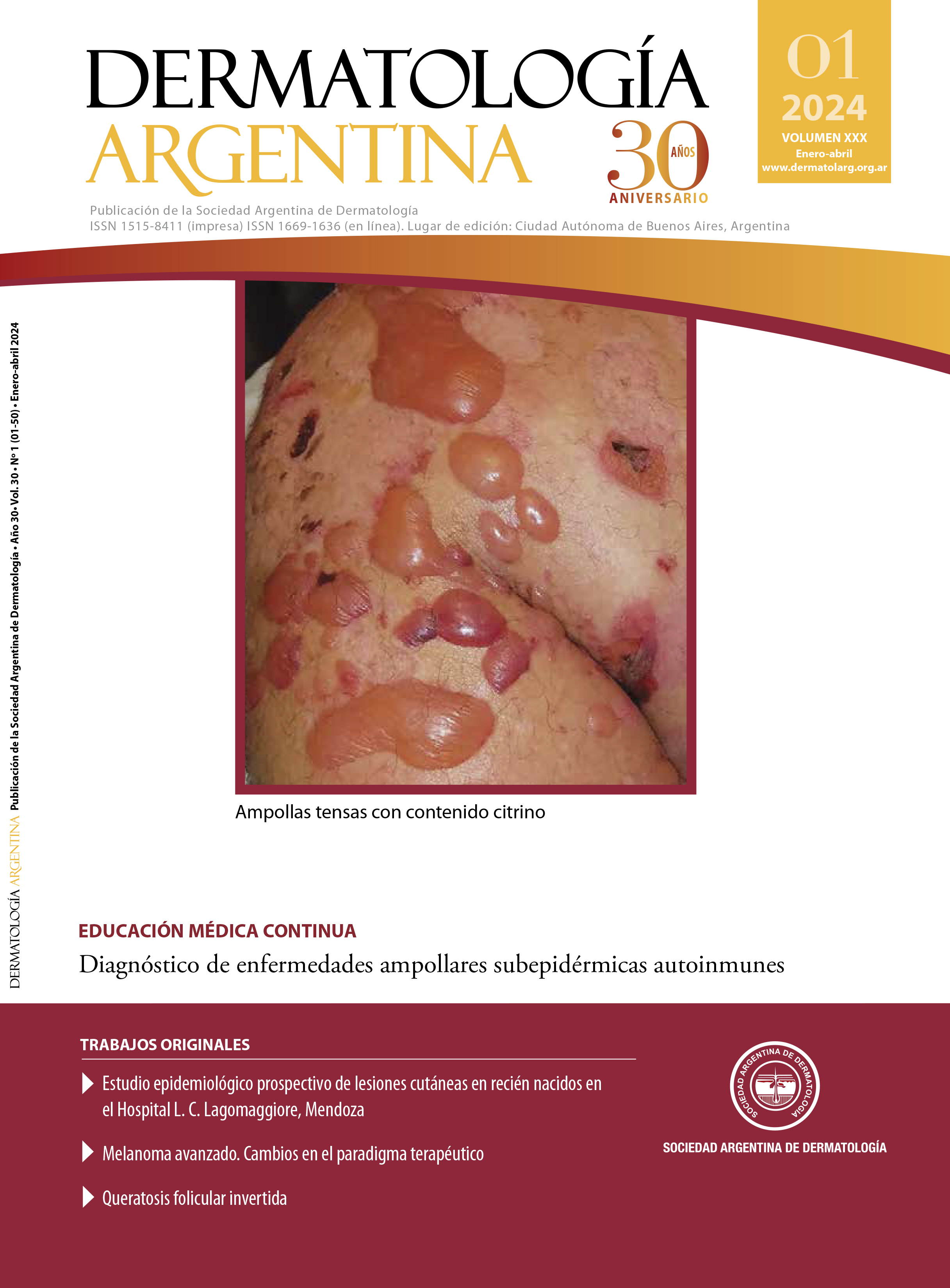
On physical examination, she presented non-follicular pustules, with an erythematoedematous base and fine scales on the surface, located on the trunk, axillae and extremities.
The laboratory reported: white blood cells of 10,000mm3 with neutrophilic predominance, blood glucose of 226 mg/dl, CRP of 20 mg/L, ESR of 30 mm/h; The rest of the laboratory, abdominal ultrasound and chest x-ray were within normal parameters.
Pathological anatomy: spongiosis; accumulation of neutrophils on the corneal layer. Small blister with disintegrated and empty wall, moderate band-like lymphocytic inflammatory infiltrate located in the superficial, perivascular and periadnexal dermis. Dilated dermal capillaries.
References
I. Szatkowski J, Schwartz R. Acute generalized exanthematous pustulosis (AGEP): a review and update. J Am Acad Dermatol. 2015;73:843-848.
II. Meneses M, Copparoni C, Samper A, Méndez D, ét al. Pustulosis exántematica aguda generalizada. Presentación de un caso y revisión de la literatura. Rev Argent Dermatol. 2012;93:3-10.
III. Laurence F, Heidemeyer K, Yawalkar N. Acute generalized exanthematous pustulosis: pathogenesis, genetic background, clinical variants and therapy. Int J Mol Sci. 2016;17:1214.
IV. Stadler P, Oschmann A, Kerl K, Maul J, ét al. Acute generalized exanthematous pustulosis: clinical characteristics, pathogenesis, and management. Dermatol. 2023;1-6.
V. Sapiaa E, Lascanob F, García P, Dastuguea M. Pustulosis exantemática aguda generalizada. Rev Hosp Niños (B. Aires). 2019;61:159-164.
VI. Castro J, Fierro E, Castro J. Acute generalized exanthematous pustulosis related to phenytoin administration. Case report. Case Reports. 2016;2:7-12.
VII. Sidoroff A, Halevy S, Bouwes-Bavinck JN, Vaillant L, et ál. Acute generalized exanthematous pustulosis (AGEP). A clinical reaction pattern. J Cutan Pathol. 2001;28:113-119.
VIII. Sidoroff A, Dunant A, Viboud C, Halevy S, ét al. Risk factors for acute generalized exanthematous pustulosis (AGEP). Results of a multinational case-control study (EuroSCAR). Br J Dermatol. 2007;157: 989-996.
IX. Chaabane A, Aouam K, Gassab L, Njim, L. ét al. Acute generalized exanthematous pustulosis (AGEP) induced by cefotaxime. Fundam Clin Pharmacol. 2010;24:429-432.
Downloads
Published
Issue
Section
License
Copyright (c) 2024 on behalf of the authors. Reproduction rights: Argentine Society of Dermatology

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
El/los autor/es tranfieren todos los derechos de autor del manuscrito arriba mencionado a Dermatología Argentina en el caso de que el trabajo sea publicado. El/los autor/es declaran que el artículo es original, que no infringe ningún derecho de propiedad intelectual u otros derechos de terceros, que no se encuentra bajo consideración de otra revista y que no ha sido previamente publicado.
Le solicitamos haga click aquí para imprimir, firmar y enviar por correo postal la transferencia de los derechos de autor